What is in-toeing? In-toeing is a term that refers to a walking pattern in which a child’s feet turn inward, […]

What is in-toeing?
In-toeing is a term that refers to a walking pattern in which a child’s feet turn inward, rather than facing forwards. You might have heard it called “pigeon-toed.” In-toeing is fairly common in children and is often a normal variation that they may outgrow with time. In most cases, both feet are affected. Children with in-toeing may experience more trips and falls when walking and running.
When does it occur?
Most parents notice their children are in-toeing at around 2-4 years of age. Research has shown up to 30% of 4 years olds demonstrate an in-toeing walking pattern. In-toeing continues to reduce as children’s bones grow and their joints develop. By 8-10 years old, most children’s intoeing has resolved.
What causes in-toeing?
There are 3 main causes of in-toeing in children: femoral anteversion, internal tibial torsion, and metatarsus adductus. We’ll break these medical terms down for you below!
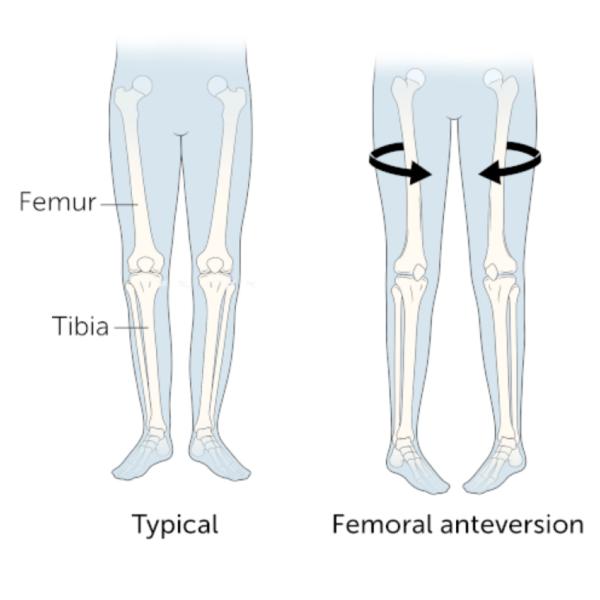
Femoral anteversion (internal femoral torsion):
Femoral anteversion, which can also be called internal femoral torsion, refers to the thigh bone rotating inwards. The foot turning inwards can actually be a result of what’s happening much higher in the leg! Children with femoral anteversion usually grow out of it by 10 years old.
Internal tibial torsion:
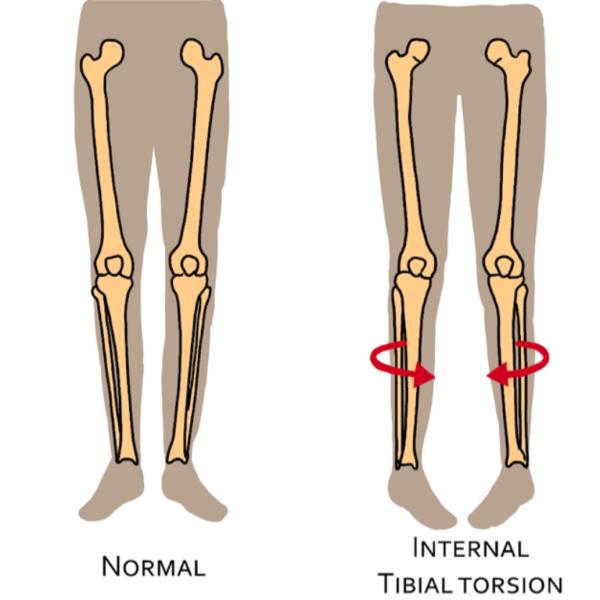
Throughout normal development, the tibia (or shin bone) experiences torsional (twisting) changes. Internal tibial torsion refers to when the bone is twisted inwards. In this instance of in-toeing, the child’s knees face forwards while their shin and foot turns inwards. This typically improves with time as their bones continue to grow and muscles get stronger, and has resolved by 8 years old in most children.
Metatarsus adductus:
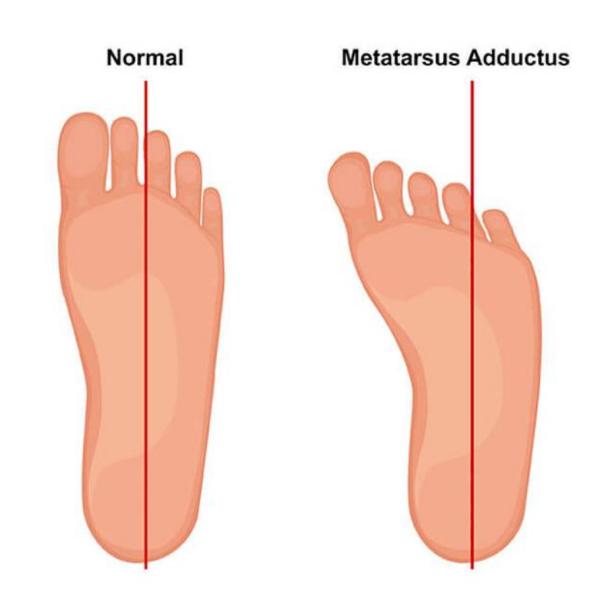
The metatarsals are the long bones in the middle of the foot. Metartarsus adductus refers to these bones curving inwards, making the outside border of the child’s foot look curved. This can occur due to the way babies were positioned in the womb. If the child’s foot can be corrected to a straight position, we call this a flexible metatarsus adductus. Children who have flexible metatarsus adductus usually don’t require treatment, it improves spontaneously by 2-3 years of age.
Does my child need to see a paediatric physiotherapist for their in-toeing?
As you’ve learned, in-toeing in children is often a normal part of development and it’s usually nothing to worry about. However, if you have concerns, it can be reassuring to see a paediatric physio. We have specialist knowledge of child development and can help rule out more serious causes of in-toeing through a thorough assessment.
There are also times when it’s important and necessary to see a paediatric physio. If your child is in-toeing and shows any of the following signs, they should be assessed by a paediatric physiotherapist:
References
Verch, R., Hirschmüller, A., Müller, J., Baur, H., Mayer, F., & Müller, S. (2018). Is in‑toing gait physiological in children? : Results of a large cohort study in 5910 healthy (pre‑)school children. Gait & Posture, 66, 70‑75. https://doi.org/10.1016/j.gaitpost.2018.08.019
The Royal Children’s hospital Melbourne https://www.rch.org.au/uploadedFiles/Main/Content/rheumatology/intoeing.pdf
NHS Inform. https://www.nhsinform.scot/illnesses-and-conditions/muscle-bone-and-joints/children-and-young-peoples-muscles-bones-and-joints/intoeing-pigeon-toe-in-children-and-young-people/
